A landmark study published in 2015 called “Learning Early About Peanut Allergy (LEAP),” revolutionized our understanding of the development of peanut allergy in children and transformed the guidance that pediatricians and allergists/immunologists give to parents about when to introduce peanut foods to children at high risk for food allergies.
Babies enrolled in the LEAP study were at high risk for developing peanut allergy because they already had severe eczema (i.e., atopic dermatitis), egg allergy, or both. Beginning at age 4-10 months, babies in the LEAP study were split into 2 groups and were followed for 4 years. One group avoided peanut foods, while the other group was given age-appropriate peanut foods several times a week. By age 5, the children who had begun eating peanut as infants were much less likely to be allergic to peanuts. Eating peanut foods early and regularly reduced the risk of peanut allergy by more than 80% compared to the group of children who avoided peanuts.
In a follow-up study called “Persistence of Oral Tolerance to Peanut (LEAP-On),” the results showed that peanut tolerance promoted by early introduction to peanut foods could be long-lasting. Children who ate peanuts from infancy to age 5 and then avoided peanuts from age 5 to age 6 were still 74% less likely to have peanut allergy than children who had consistently avoided peanut foods from infancy to age 6.
Does introducing allergenic foods early in life put a baby at a greater risk for food allergy?
A study published in 2016, called the “Enquiring About Tolerance (EAT)” study randomly assigned 1,300 breastfed infants to 1 of 2 treatment groups at age 3 months. One group was introduced to a sequence of 6 allergenic foods (i.e., milk, peanut, egg, sesame, fish and wheat), while the other group continued breastfeeding exclusively until age 6 months.
The EAT study revealed that rates of allergy to the 6 foods were not significantly different when the early introduction group and the exclusively breastfed group were compared at ages 1 and 3. This showed that early introduction of allergenic foods did not increase a baby’s risk for food allergy.
Does early introduction of egg products reduce the risk of developing egg allergy too?
In 2019, a new analysis of the EAT study data showed that early introduction of allergenic foods did protect against food allergies for some children at high risk. Children were considered at high risk if their blood tests showed specific IgE antibodies to the foods. They were considered sensitized. These specific IgE antibodies mediate allergic reactions.
Compared to exclusive breastfeeding, early food introduction reduced the likelihood that a baby would be sensitized to 1 or more of the 6 foods. It also made it less likely for the baby to develop an allergy to 1 or more of the 6 foods.
Early introduction of peanuts lowered the risk of developing peanut allergy in babies sensitized to peanuts. This finding is consistent with the LEAP study.
Early introduction of egg lowered the risk of developing egg allergy in babies sensitized to egg. Early introduction of foods including egg also provided protection against egg allergy in babies with moderate or severe eczema at age 3 months.
For babies who were not sensitized to any of the 6 foods at the beginning of the study, the risk of developing an allergy to 1 or more of the foods was similar in both the early introduction and exclusive breastfeeding groups.
These new findings from the EAT study indicate that early introduction of egg can provide protection against egg allergy for at least some children at high risk for developing egg allergy.
Guidance from American Academy of Allergy, Asthma & Immunology (AAAAI), American College of Allergy, Asthma & Immunology (ACAAI), and the Canadian Society for Allergy and Clinical Immunology:
To prevent peanut and/or egg allergy, both peanut and egg should be introduced around 6 months of life, but not before 4 months. Screening before introduction is not required. Other food allergens should be introduced around this time as well. Upon introducing complementary foods, infants should be fed a diverse diet, because this may help foster the prevention of a food allergy. Maternal exclusion of common allergens during pregnancy and/or lactation as a means to prevent food allergy is not recommended.
The board certified allergy doctors of Black & Kletz Allergy have had over half a century of experience dealing with food allergies in both children and adults. Black & Kletz Allergy has 3 office locations in the greater Washington, DC, Northern Virginia, and Maryland metropolitan area. The allergists at Black & Kletz Allergy diagnose and treat individuals with allergies (e.g., hay fever, food allergies, medication allergies), asthma, hives, swelling episodes, eczema, contact dermatitis, insect bites, bee sting allergies, sinus disease, and immunologic problems. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA and have on-site parking at each location. The Washington, DC and McLean, VA offices are Metro accessible and there is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. Please call us to make an appointment or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. Black & Kletz Allergy has been striving to provide high quality allergy and asthma care to the residents of the Washington, DC metro area for more than 50 years. We are committed to continue delivering state-of-the-art allergy and asthma care in the future.
Christmas tree syndrome is a relatively new term that is used to describe allergies to Christmas trees, whether they are real or artificial. The allergen can be the tree itself or it can be something that is on the surface of the tree.
Symptoms:
The symptoms of Christmas tree allergy are the same symptoms that an individual gets with classic cases of allergic rhinitis (i.e., hay fever) and/or allergic conjunctivitis (i.e., eye allergies). These symptoms may include sneezing, runny nose, nasal congestion, post-nasal drip, itchy nose, itchy throat, itchy eyes, watery eyes, redness of the eyes, sore throat, sinus congestion, sinus headaches, fatigue, and/or snoring. In individuals with asthma, Christmas trees may also exacerbate asthma symptoms such as chest tightness, wheezing, coughing, and/or shortness of breath.
Causes:
The causes of Christmas tree syndrome may include the pine pollen of the actual Christmas tree itself. It should be noted that pine pollen is fairly heavy and is not typically a major tree allergen when you compare it with other tree pollens such as maple, oak, elm, hickory, birch, etc. Despite it being less allergenic than other tree pollens, pine pollen can still however cause allergic rhinitis symptoms in sensitive individuals.
Natural Christmas trees are also known to carry more than 50 types of mold. Three-quarters of these molds are known to cause allergic rhinitis symptoms. It is also known that having a natural Christmas tree in one’s house will increase the amount of indoor mold since mold levels are higher in a room with a real Christmas tree as opposed to a room without a Christmas tree. Natural Christmas trees can also contain animal urine, pine tree sap, pesticides, insect droppings, and pollutants on them which may cause allergy-type symptoms in certain individuals. The scent of the terpenes found in pine tree sap can also trigger allergy symptoms, even though it is not technically an allergen, but rather an irritant.
Artificial Christmas trees may also have high levels of molds, but often have high levels of dust associated with them. Artificial Christmas trees also are often stored in dusty areas for prolonged periods of time. The dust that gathers on the surface of the trees may then play havoc with a sensitive person’s allergies. In addition, artificial Christmas trees may harbor insects, insect droppings, rodent urine, and rodent droppings which all may act as allergens that cause miserable allergy symptoms.
In addition to the Christmas tree itself, the decorations (e.g., ornaments, tinsel, garland, strings of lights, ribbon, pine cones, scented candles, poinsettias and other Christmas plants) may also possess allergens that may cause allergy symptoms.
Treatment:
The treatment of Christmas tree syndrome is to first remove the individual from the area in the house where the Christmas tree is located. Unfortunately, this is usually not possible because Christmas is a time to be with family members and most of the time that involves being in the room with the tree. If one is unable or unwilling to avoid exposure to the Christmas tree, one can use a variety of allergy medications to help alleviate the allergy symptoms. Oral antihistamines, oral decongestants, nasal corticosteroids, and/or nasal antihistamines are usually the initial treatment modalities in most allergic individuals. If other medications are needed, nasal anticholinergics and/or oral leukotriene antagonists can also be utilized.
Prevention:
Obviously, the prevention of Christmas tree exposure has the best outcome, but in the holiday spirit, the following things can help alleviate allergy symptoms in individuals who plan on putting up a Christmas tree. Some of the recommendations for minimizing allergy symptoms with Christmas trees may include cleaning the tree, keeping the tree outside, increase the ventilation of the room, minimize exposure to the tree, and/or use an alternative instead of a tree such as a Christmas “statue.” Christmas “candy cane,” etc.
The board certified allergy specialists at Black & Kletz Allergy have 3 convenient locations in the Washington, DC, Northern Virginia, and Maryland metropolitan area and we have been providing allergy and asthma care to this area for more than 50 years whether it is Christmas or not. Our offices are located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All of our offices offer on-site parking. For further convenience, our Washington, DC and McLean, VA offices are Metro accessible. In addition, our McLean, VA office location offers a complementary shuttle that runs between this office and the Spring Hill metro station on the silver line. For an appointment, please call one of our offices. Alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. If you suffer from allergies or asthma, it is our mission to help alleviate your undesirable symptoms, so that you can enjoy a better quality of life. Black & Kletz Allergy is dedicated to providing the highest quality allergy and asthma care in an empathetic, relaxed, and professional environment.
Many patients who experience seasonal allergic rhinitis (i.e., hay fever) and allergic conjunctivitis (i.e., eye allergies) symptoms (e.g., sneezing, runny nose, nasal congestion, post-nasal drip, sinus congestion, itchy nose, itchy throat, sinus headaches, itchy eyes, watery eyes, redness of the eyes) caused by sensitivities to tree, grass, and weed pollens also may experience an itchy mouth and throat after eating certain fresh fruits and vegetables. As the symptoms are usually limited to the mouth and throat, this condition is known as “pollen food allergy syndrome” (PFAS). It is also known by the name “oral allergy syndrome” (OAS).
Most people with food pollen allergy syndrome have oral symptoms such as itching, burning, tingling, and occasionally swelling of the lips, mouth, tongue, and/or throat where the fresh fruit or vegetable touches the mouth. This represents a form of contact urticaria, since there is direct contact of the food to the mouth region. The symptoms usually only last a matter of seconds to a few minutes. The symptoms are also more likely to occur in the season that the cross-reactive pollens are also prevalent.
The oral symptoms occur only when a pollen-allergic individual is exposed to raw or fresh vegetables, fruits, and/or nuts. Food pollen allergy syndrome typically does not occur with cooked or baked fruits, vegetables, or processed fruits such as in applesauce as the cooking process inactivates or denatures the protein allergens in the foods. The exception to this rule is with celery and nuts where the oral allergy symptoms typically occur even if they have been cooked.
The cause for food pollen allergy syndrome is thought to be a cross-reactivity between the protein allergens in the pollen and the fresh fruits and/or vegetables. Fruit and vegetable proteins (i.e., allergens) share varying degrees of structural similarities with allergens found in pollens as well as other fruits and vegetables. This structural homology confuses the immune system and causes an allergic reaction to occur. The patient’s body “sees” the fruit or vegetable protein allergen as the pollen allergen and reacts to the food because it “thinks” it is the pollen. This homology or similarity between the food allergen and the pollen allergen is referred to as cross-reactivity.
Certain pollens are more likely to be cross-reactive with certain fruits, vegetables, and/or nuts. Below is a list of the cross-reactivity that may occur between common pollens and common raw or fresh fruits, vegetables, and/or nuts:
Note: Any of the above pollens may cross-react with berries (e.g., strawberries, blueberries, raspberries), citrus (e.g., oranges, lemons), grapes, mango, fig, peanut, pineapple, pomegranates, and/or watermelon.
When a fruit or vegetable allergy develops in the absence of a pollen allergy, patients may be sensitized to nonspecific lipid transfer proteins (nsLTPs) or to gibberellin-regulated proteins (GRPs). In general, sensitization to these proteins is associated with higher rates of systemic reactions as well as higher rates of food-dependent, exercise-induced anaphylaxis. The allergens responsible for isolated food allergy are typically resistant to both heat and digestion and therefore have a greater potential to cause systemic symptoms.
There are also several syndromes that are associated with pollens and foods:
Celery-mugwort-birch-spice syndrome — The celery-mugwort-birch-spice syndrome is a potentially severe form of celery allergy seen in children and adults who are sensitized to both birch and mugwort pollens. Patients with this syndrome react to celeriac (i.e., root of the celery plant or celery tuber).
Mugwort-pollen food allergy syndrome — Patients sensitized to mugwort (Artemisia vulgaris) may develop a systemic food allergy (e.g., to mustard).
Latex-fruit syndrome — Approximately 30-50% of individuals who are allergic to natural rubber latex show an associated hypersensitivity to some plant-derived foods, especially fresh fruits. An increasing number of plant foods, such as avocado, banana, bell pepper, chestnut, kiwi, peach, tomato, and white potato, have been associated with this syndrome.
Diagnosis: The diagnosis is suspected when a comprehensive history is suggestive of pollen food allergy syndrome. Allergy tests such as prick skin testing, food elimination, and oral food challenges are helpful in establishing the diagnosis. Food prick skin testing with fresh foods is more reliable than commercial extract food prick skin testing because the process of making the extract can destroy the responsible protein allergen.
Treatment: The treatment of pollen food allergy syndrome involves avoiding exposure to the involved fresh or raw fruits, vegetables, and/or nuts to prevent the uncomfortable feeling in the mouth and throat, as well in order to reduce the risk of rare systemic symptoms. Taking antihistamines can minimize the severity of the symptoms however systemic reactions need treatment with epinephrine injections. Patients with a history of a systemic reaction should be prescribed a self-injectable epinephrine device (e.g., EpiPen, Auvi-Q, Adrenaclick) and instructed on when and how to use it. It is important that the patient go immediately to the closest emergency room once a self-injectable epinephrine device is used.
The board certified allergy doctors at Black & Kletz Allergy will eagerly respond to your needs for further information and services in dealing with food allergies, pollen food allergy syndrome, and other allergic and immunologic disorders. The allergists at Black & Kletz Allergy have 3 convenient locations in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Our offices are located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. We offer on-site parking at all of our offices and our Washington, DC and McLean, VA offices are Metro accessible. There is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. To make an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond to your inquiry within 24 hours by the next business day. Black & Kletz Allergy treats both adults and children and we strive to provide the best and most current diagnostic and treatment modalities in the Washington, DC metro area, as we have done for more than 5 decades.
Corn (i.e., maize) is a popular staple food worldwide, providing essential nutrients such as vitamins, minerals, and fiber. Corn is also a common component of processed foods. Despite its nutritional value and popularity, for those individuals with corn allergies or corn intolerance, consuming corn or corn-derived products may lead to adverse health effects.
Although corn allergies and intolerance are relatively uncommon compared to other food allergies and intolerances, they can still cause significant discomfort and health issues for affected individuals.
Corn allergies are caused by an overreaction of the immune system to proteins found in corn whereas corn intolerance typically results from the body’s inability to digest or process corn.
Corn Allergy:
There may be a genetic predisposition to developing a corn allergy, as it is more common in individuals with a family history of allergies or other allergic conditions, such as asthma or eczema (i.e., atopic dermatitis). Corn allergy is not a very common food allergy. The prevalence of corn allergy is approximately 2% in whites, 7% in Hispanics, and 15% in African Americans. Corn allergy occurs when the immune system mistakenly identifies corn proteins as harmful substances. As a result, an allergic reaction ensues against the corn protein. In this allergic reaction, the body produces immunoglobulin E (IgE) antibodies which trigger the release of chemical mediators such as histamine, leukotrienes, prostaglandins, as well as other inflammatory chemicals. In doing so as a mechanism to “kill” or “get rid of” the allergen (e.g., corn protein), the individual experiences classic allergy symptoms such as itching (i.e., pruritus), hives (i.e., urticaria), swelling (i.e., angioedema), gastrointestinal symptoms, wheezing, shortness of breath, or anaphylaxis.
Zein is the major storage protein found in corn. It makes up about 45% of the protein in corn. Zein is used as a coating for nuts, pills, candy, fruit, as well as other encapsulated foods and medications. In addition to zein, lipid transfer protein and profilin are two other proteins that are found in corn. These 2 proteins are primarily responsible for most of the corn allergy that occurs. Allergies to the heat-stable lipid transfer protein in corn may cause severe allergic reactions whereas an allergy to the heat-sensitive profilin protein usually only cause mild to moderate reactions.
Symptoms:
Mild to moderate corn allergy symptoms may include sneezing, itchy mouth, itchy throat, runny nose, nasal congestion, post-nasal drip, generalized itching, hives, and/or gastrointestinal issues such as nausea, vomiting, and/or diarrhea.
In rare instances, corn allergy may lead to anaphylaxis, a severe and potentially life-threatening allergic reaction. The symptoms of anaphylaxis may include hives, swelling of the throat or tongue, wheezing, shortness of breath, rapid or weak pulse, and/or a sudden drop in blood pressure.
Diagnosis:
The diagnosis of corn allergy requires a thorough history of the timeline of consumption of the corn-containing food(s) and the symptoms experienced. The diagnosis can be confirmed by identification of corn specific IgE antibodies either by skin prick testing or by blood testing. The gold standard for establishing the diagnosis of corn or any other food allergy however is an oral food challenge.
Corn allergy may be associated with cross-reactivity to other food allergens such as certain grains, legumes, and seeds. A high degree of cross-reactivity has been demonstrated among the lipid transfer proteins of corn (maize), peach, apple, apricot, walnut, hazelnut, peanut, rice, sunflower seeds, and French beans. This cross-reactivity means that individuals with a corn allergy may also experience allergic reactions to other foods containing similar proteins.
Occupational exposure to maize, maize dust, or maize flour may result in occupational asthma or rhinitis, in particular in mill workers, bakery workers, and those working in the animal feed industry. Allergic reactions have also been reported to cornstarch powder when used as a glove lubricant. Symptoms include hives, swelling episodes, sneezing, runny nose, nasal congestion, post-nasal drip, itchy eyes, watery eyes, redness of the eyes, asthma, and/or intermittent episodes of shortness of breath.
Corn has been implicated as one of the foods that can cause eosinophilic esophagitis, a disorder with symptoms suggestive of gastroesophageal reflux disease (GERD) but unresponsive to conventional anti-reflux therapies.
Treatment:
The treatment of corn allergy usually includes the use of antihistamines. Antihistamines can relieve the mild symptoms of allergic reactions such as itching and rashes. Severe reactions such as anaphylaxis usually require epinephrine injections either with a syringe and a needle or with a self-injectable epinephrine device (e.g., EpiPen, Auvi-Q, Adrenaclick). It should be noted that if an individual uses a self-injectable epinephrine device, they must go immediately to the closest emergency room.
Prevention:
The avoidance of foods containing corn products is the only definitive preventive measure. It is essential to read food labels carefully, as corn-derived ingredients can be found in various foods under different names, such as cornstarch, corn syrup, dextrin, and maltodextrin. It is essential to be vigilant about identifying hidden sources of corn and choosing alternative products when necessary. Corn may be present in salad dressings, sauces, processed meats, and in certain medications and supplements.
Corn Intolerance:
Certain enzymes such as amylase are necessary to break down complex carbohydrates into simple digestible sugars. The deficiency of these enzymes can result in bothersome gastrointestinal symptoms such as abdominal bloating, cramping, abdominal pain, and diarrhea after consuming corn products.
Sensitivity to specific corn components, such as cornstarch or corn syrup, may also contribute to corn intolerance. Though less common, intolerance can also result in skin manifestations such as rashes and itching, as well as respiratory symptoms such as cough, chest tightness, wheezing, and/or shortness of breath.
Corn is a low FODMAP food. FODMAP stands for fermentable oligosaccharides, disaccharides, monosaccharides and polyols. Foods high in FODMAPs may cause symptoms of food intolerance, thus affecting the gastrointestinal system. These symptoms of intolerance however can be mistaken for a true food allergy. Note that even though corn is a low FODMAP food, corn syrup, on the other hand is a high fructose food and thus considered a high FODMAP food.
Corn, like other grains, contains a moderate amount of lectins. Lectins are another cause of food intolerance. Cooking foods with lectins makes them more digestible and can reduce the symptoms of food intolerance however.
Corn allergy has been associated with a condition called “latex food syndrome.” The syndrome occurs when an individual who has a latex eats a food that has proteins in it that are similar to the proteins found in latex. The rubber tree plant Hevea brasiliensis which is involved in latex allergy, has an allergen called Hev b 11 which is a chitinase protein. Many plant and animal tissues contain chitinase proteins which are allergenic. Corn, kiwi, chestnut, mango, banana, avocado, pomegranate, and dates all contain chitinase proteins. Those that are sensitized to latex may have allergic reactions from foods containing similarly shaped proteins. Approximately 30% to 50% of individuals with latex allergies have a cross-reaction to foods with these proteins. The symptoms are primarily oral symptoms (e.g., itchy mouth, lips, tongue and throat) and are often referred to as oral allergy syndrome or pollen food allergy syndrome. Oral allergy syndrome mostly affects people who already suffer from pollen allergies and seasonal allergic rhinitis.
Prognosis:
Healthcare professionals, patients, and caregivers all play a vital role in the successful management of corn intolerance and allergies. Working together to identify triggers, develop individualized management plans, and provide ongoing support can help ensure that individuals with corn allergies or intolerance can live healthy and fulfilling lives.
If you suffer from a corn allergy or other food allergy or intolerance of any kind, the board certified allergists at Black & Kletz Allergy have the expertise in order to diagnose and manage this condition. We treat both pediatric and adult patients and have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. We have on-site parking at each location and both the Washington, DC and McLean, VA offices are Metro accessible. Please either call us for an appointment or you may alternatively click Request an Appointment and we will respond within 24 hours by the next business day. The allergy specialists at Black & Kletz Allergy have been treating allergy, asthma, and immunology patients in the Washington, DC metropolitan area for more than 5 decades and we strive to provide state-of-the-art allergy care in a professional and amiable setting.
Snoring is not an uncommon symptom in patients with allergic rhinitis (i.e., hay fever). Snoring is the harsh sound that arises when air flows past the relaxed tissues in the throat. The actual snoring sound is a result of the vibration of the throat’s tissues as one breathes. Mild intermittent snoring is quite common and occurs in almost everyone. Chronic moderate or severe snoring however is not normal and may indicate a serious health malady. It may also point to an underlying health condition such as sleep apnea, allergic rhinitis, nasal polyps, obesity, enlarged tonsils, etc.
Sleep apnea is a condition in which one’s breathing is continually interrupted. The result is the inability to get enough deep sleep that is essential to revitalize the body. The characteristic symptoms of this condition include extreme daytime somnolence which often results in falling asleep at inappropriate times. Sleep apnea should not be taken lightly as it can be very serious and is a potentially fatal disorder. In addition to falling asleep and daytime sleepiness, other symptoms may include snoring (as mentioned above), fatigue, depression, diminished productivity at work and/or school, decreased memory, decreased quality of life, and a reduced ability to learn. As mentioned above, allergic rhinitis (i.e., hay fever) has also been linked to many of the same symptoms. Allergic rhinitis in combination with sleep apnea can have harmful effects including heart disease, stroke, sexual dysfunction, and an increased risk for motor vehicle accidents. As a result, sleep apnea should be taken seriously. Although it is estimated that roughly 25 million adults in the U.S. have sleep apnea. The actual numbers are probably much higher since cases are underdiagnosed due to a variety of reasons. In addition, many individuals with sleep apnea are simply unaware that they have the condition.
There are 2 types of sleep apnea, “obstructive sleep apnea” and “central sleep apnea.” In obstructive sleep apnea, the breathing or air flow is blocked or “obstructed.” The obstruction is often caused by the tongue sliding back in the throat. In addition, the relaxed airway that occurs during sleep changes shape to a more oval shape. This change in shape of the airway contributes to the decrease in air that reaches the lungs. In essence, the muscles of the throat relax and fail to hold the airway open during sleep. As a result, oxygen levels are decreased in the tissues. In central sleep apnea, the normal unconscious breathing basically stops, usually due to the brain not sending the normal signals to the muscles that control breathing. Central sleep apnea is much less common than the obstructive type of apnea and not associated with allergies. For the purposes of this blog article, only obstructive sleep apnea is discussed.
The severity of the sleep apnea can be put into 3 categories: mild, moderate, and severe. The severity is based on the number of episodes or events of apnea that occur per hour of sleep. An episode or event is described as a complete stoppage of breathing for at least 10 seconds or shallow breaths for at least 10 seconds. Sleep apnea is considered “mild” when there are 5-14 episodes of apnea or hypopnea (i.e., shallow breathing) per hour. It is deemed “moderate” when there are 15-29 episodes of apnea or hypopnea per hour. It is called “severe” when there are 30 or more episodes of apnea or hypopnea per hour.
The diagnosis of sleep apnea is best done with a sleep study. Historically, patients were asked to come to a sleep center for an overnight sleep study. During the sleep study the individual’s blood pressure, heart rate, respiratory rate, oxygenation level, and brain electrical activity is monitored throughout the night. More recently, the sleep study is often done in the patient’s home with some of these measures closely monitored and recorded. In addition allergy skin testing or blood testing may be performed in individuals exhibiting allergic rhinitis symptoms. Some of these symptoms may include sneezing, itchy nose, runny nose, nasal congestion, post-nasal drip, snoring, sinus pressure, sinus headaches, fatigue, itchy throat, itchy eyes, watery eyes, and/or redness of the eyes.
The most efficacious management of sleep apnea is the use of CPAP (continuous positive airway pressure) while sleeping. CPAP machines are used in order to deliver a continuous flow of pressure which as a result forces open the obstruction in the airway. The patient has 3 options how to receive the continuous airflow delivered by the CPAP machine which includes a full face mask, a nasal mask, or nasal pillows or prongs. The full face mask is the most cumbersome whereas the nasal pillows or prongs are the least awkward. The choice is completely up to the patient and many individuals try all 3 until they find the best match for themselves. It should be pointed out that the main obstacle in the treatment of sleep apnea is compliance, as more than half of patients do not use CPAP when prescribed, mostly due to it being uncomfortable and annoying.
The use of dental or mouth devices are controversial but may help lessen symptoms in patients with mild obstructive sleep apnea. Surgery can also be performed in order to improve obstructive sleep apnea. The “Inspire Sleep Apnea Innovation” is a form of upper airway stimulation (UAS). It is a surgical procedure in which a monitoring device is implanted into one’s chest and a neurostimulator device is implanted below one’s chin in order to monitor one’s breathing and send a gentle pulse to the nerve that controls tongue motor function, moving it forward and out of the way so one can breathe properly. This treatment received FDA approval in 2014. Other surgical procedures are somewhat controversial in regards to their efficacy. One of these is a uvulopalatopharyngoplasty which is one of the most common surgical procedures for treating obstructive sleep apnea, although as mentioned above, not necessarily the most effective. It is performed to remove excess tissue in the throat such as the uvula, adenoids, tonsils, and parts of the soft palate.
Black & Kletz Allergy has 3 convenient locations with on-site parking located in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. The Washington, DC and McLean, VA offices are Metro accessible and we offer a free shuttle that runs between the McLean, VA office and the Spring Hill metro station on the silver line. The board certified allergy doctors at Black & Kletz Allergy are extremely knowledgeable regarding the diagnosis and treatment of snoring and sleep apnea. In our practice we also treat patients with environmental allergies (i.e., allergic rhinitis or hay fever), eye allergies (allergic conjunctivitis), asthma, eczema (i.e., atopic dermatitis), hives (i.e., urticaria), contact dermatitis, medication allergies, generalized itching (i.e., pruritus), swelling episodes (i.e., angioedema), insect sting allergies, food allergies, eosinophilic esophagitis, Mast cell disorders, and immune disorders. To schedule an appointment, please call any of our offices or you may click Request an Appointment and we will respond within 24 hours by the next business day. We have been serving the greater Washington, DC metropolitan region for more than 50 years and we look forward to providing you with exceptional allergy care in a welcoming and professional environment.
The Eustachian tube is a small canal that connects the middle ear to the back of the nose and upper throat. It is normally closed but opens when we swallow, yawn, or chew.
Normal functions of the Eustachian tube:
Ventilation of the middle ear – Helps keep the air pressure equal on either side of the eardrum (i.e., tympanic membrane), enabling the eardrum to work and vibrate correctly.
Drainage of secretions from the middle ear cleft.
Protection of the middle ear from pathogens (e.g., bacteria, viruses, fungi)
Dysfunction of the Eustachian tube or Eustachian tube dysfunction (ETD) may occur when the mucosal lining of the tube is swollen or does not open or close appropriately.
Causes:
1. Allergic rhinitis (i.e., hay fever) – Seasonal or perennial in nature
Upper respiratory tract infections (URI’s) – Single or recurrent episodes
Nasal septal deviation (i.e., deviated septum)
Cleft palate
Enlarged adenoids and/or tonsils – Especially in children
Feeling of clogging, fullness or pressure in the ear(s)
Pain or discomfort in the ear(s)
Muffled or decreased hearing
Ringing sensation in the ear(s)
Dizziness, vertigo, or feeling of imbalance
Complications:
Otitis media with effusion (i.e., glue ear)
Middle ear atelectasis (i.e., retraction of the eardrum)
Chronic otitis media
Diagnosis:
The inability to “clear” or “pop” the ear with changes in barometric pressure, together with other patient-reported symptoms (e.g., aural fullness, pain, muffled hearing) is consistent with Eustachian tube dysfunction.
Tests:
Otoscopy
Tympanometry
Nasal endoscopy
Treatment:
Non-Surgical:
Supportive care – Includes advice about self-management such as to swallow, yawn, or chew. These measures are especially useful while flying as sudden changes in barometric pressures aggravate Eustachian tube dysfunction.
Pressure equalization methods – A technique where the Eustachian tube is reopened by raising the pressure in the nose. This can be accomplished by forced exhalation against a closed mouth and nose which is referred to as the Valsalva maneuver. Blowing balloons is also helpful in relieving the pressure in the middle ear by forcing air into the Eustachian tubes and keeping them patent.
Nasal douching – The nasal cavity is washed with a saline solution in order to flush out excess mucus and debris from the nose and sinuses.
Decongestants, antihistamines, nasal or oral corticosteroids – These medications are aimed at reducing nasal congestion and/or inflammation of the lining of the Eustachian tube.
Antibiotics – Used for the treatment of rhinosinusitis (i.e., sinus infections)
Simethicone – This is currently being investigated in adults to assess whether or not it can help to break up bubbles that may block the opening of the Eustachian tube in the back of the nose during an upper respiratory infection. As a result, air should be able to pass between the nose and middle ear easier.
Surgical:
Insertion of a pressure equalizing tube into the eardrum – Also known as a tympanostomy tube, ventilation tube, or grommet. Pressure equalizing tubes typically fall out of the ears after 6-9 months.
Eustachian tuboplasty – Balloon dilatation of the Eustachian tube
Of note: The opposite condition of Eustachian tube dysfunction is called patulous Eustachian tube. In this malady, there is an abnormal patency of the Eustachian tube. Instead of being in the normal closed position, the Eustachian tube stays intermittently open, causing an echoing sound of the person’s own heartbeat, breathing, and/or speech. These sounds will then vibrate directly onto the eardrum causing a “bucket on the head” sound effect. This condition can usually be managed by nasal sprays. Rarely, surgical intervention is warranted.
The board certified allergists at Black & Kletz Allergy has 3 locations in the Washington, Northern Virginia, and Maryland metropolitan area. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. All 3 of our offices have on-site parking and the Washington, DC and McLean, VA offices are Metro accessible. The McLean office has a complementary shuttle that runs between our office and the Spring Hill metro station on the silver line. The allergy specialists of Black & Kletz Allergy diagnose and treat both adult and pediatric patients. For an appointment, please call our office or alternatively, you can click Request an Appointment and we will respond within 24 hours by the next business day. The allergy specialists at Black & Kletz Allergy have been helping patients with Eustachian tube dysfunction, allergic rhinitis (i.e., hay fever), asthma, sinus disease, eczema (i.e., atopic dermatitis), hives (i.e., urticaria), insect sting allergies, immunological disorders, medication allergies, and food allergies for more than 50 years. If you suffer from allergies, it is our mission to improve your quality of life by reducing or preventing your undesirable and annoying allergy symptoms.
The term “chronic sinusitis” is defined as an inflammation of the sinus or sinuses lasting more than 12 weeks in duration. The inflammation can be of any etiology however it is implied and commonly agreed upon that infection is the primary cause of chronic sinusitis. In order to understand chronic sinusitis, it is important to know the anatomy of a sinus. A sinus is a cavity in any organ or tissue, but in reference to allergies, it is a cavity in the skull and often referred to a “paranasal sinuses.” There are 4 paired sinuses in the cranial bones. They are named for their location with regards to the head and face. The names of the sinuses include the frontal, ethmoid, sphenoid, and maxillary sinuses. The frontal sinuses are located in the forehead region above the eyes. The ethmoid sinuses are situated between the eyes on each side of the upper nose. The sphenoid sinuses are positioned behind the eyes and bridge of the nose and lie in the deeper areas of the cranium. The maxillary sinuses are located on either side of the nostrils in the cheekbone areas.
The symptoms of inflammation of the sinuses or a chronic sinus infection may include a sinus headache, facial pressure or pain, post-nasal drip, discolored nasal secretions, cough and/or fatigue. It should be noted that it is not uncommon for an individual to present with just a chronic cough without many additional sinus symptoms. The diagnosis of chronic sinusitis requires a comprehensive and physical examination. There is often a history of onset of the infection as well as a progression of specific symptoms which may help diagnose the sinus infection. In some instances, sinus X-rays and/or CT scans of the sinuses may be helpful in the diagnosis.
The treatment of chronic sinusitis varies depending upon how severe the symptoms are in each individual patient. Oral antibiotics are the most common treatment however a longer course of antibiotics is usually prescribed due to the chronicity of the infection. It is not uncommon to treat these patients with 30 days of continuous oral antibiotics. Topical corticosteroids [e.g., Flonase (fluticasone), Nasonex (mometasone), Nasacort AQ (triamcinolone), Rhinocort (budesonide), Qnasl (beclomethasone), Nasarel (flunisolide), Zetonna (ciclesonide), (Xhance (fluticasone)] are sometimes useful in the local treatment of bacterial infections. The effects are usually short-lived however. The nasal corticosteroids are not currently recommended for routine use; however, they offer the potential for improved directed treatment of the sinuses. Saline irrigation or saline nasal strays are useful in the mechanical clearance of allergens, irritants, and microorganisms (i.e., bacteria, viruses) from the nasal and sinus cavities. Saline irrigation is an inexpensive and easy to use method of “cleaning” the nasal and sinus cavities. It is often used in conjunction with other treatments such as nasal corticosteroids and oral antibiotics to treat chronic sinusitis. It should be noted that some individuals do not like saline irrigation as it may cause some discomfort in the nasal or sinus passages. Topical antibiotics are sometimes useful in the local treatment of bacterial infections. As with nasal corticosteroids, the effects are usually short-lived and topical antibiotics are not currently recommended for routine use; however, they offer the potential for improved directed treatment of the sinuses.
Occasionally, a more aggressive treatment regimen for chronic sinusitis is necessary and other medications are then utilized. Oral corticosteroids are implemented in more severe or recalcitrant cases. Oral corticosteroids reduce inflammation and are particularly useful for shrinking nasal polyps, though they also may result in the multisystem improvement of symptoms. Nasal polyps (i.e., nasal polyposis) are soft, benign growths that develop from the lining of the sinuses and nasal cavity. Approximately 4-5% of the general population has nasal polyps. Nasal polyps cause increased nasal congestion and may block the normal drainage pattern of the sinuses. As a result, sinus infections are more likely to develop in these individuals. It should be pointed out that oral corticosteroids carry a risk for significant systemic side effects such as weight gain, peptic ulcers, cataract formation, thinning of one’s bones, depression, and/or endocrine dysfunction. They should be used judiciously and only for brief periods of time. In addition to oral corticosteroids, biological medications [i.e., Dupixent (dupilumab)] are being used more often to treat chronic sinusitis with nasal polyps. Biological medications can offer targeted and more effective treatment than other therapies. The potential advantages of biological medications include the reduced need for oral or topical corticosteroids as well as the need for sinus surgery. A few of these biological agents [i.e., Xolair (omalizumab), Fasenra (benralizumab), Nucala (mepolizumab), Dupixent (dupilumab)] are currently being used for the control of asthma but only one of them, Dupixent (dupilumab) has been approved for chronic sinusitis with nasal polyps.
Prevention is always the goal in any malady if at all possible. For chronic sinusitis, preventive measures include the identification of specific allergen sensitivities and the subsequent avoidance or preventive treatment for these allergies. Allergy testing should be done by skin testing or blood testing. Aggressive treatment of any seasonal or perennial allergic rhinitis (i.e., hay fever) promotes proper sinus drainage and as a result improves upper airway function. Allergy immunotherapy (i.e., allergy shots, allergy injections, allergy desensitization, allergy hyposensitization) is a very effective tool to treat allergies and asthma as it works in 80-85% of patients that take them. The average treatment length of allergy shots is typically 3-5 years.
Allergic reactions to sesame are increasing in incidence over the past several years. Sesame is the 9th most common food allergy among children and adults. Approximately 0.23% of the U.S population are allergic to sesame. Although 0.23% seems like a small number, the National Institute of Health’s (NIH) researchers estimate that 17% of food-allergic children have a sesame allergy.
In the past, according to the Center for Science in the Public Interest, only 14 out of 22 major food companies clearly labeled sesame ingredients on their product labels. However, on April 23, 2021, the FASTER (Food Allergy Safety, Treatment, Education, and Research) Act was passed into law. This law requires that sesame be labeled on all packaged foods in the United States. This sesame labeling began earlier this year on Jan. 1, 2023.
Sesame joins the 8 other foods that are already declared as major food allergens by federal law. The 9 major food allergens are as follows:
The protein that is contained in sesame seeds, sesame oil, tahini, etc. binds to the specific antibodies in one’s serum and causes reactions that cause the release of histamine and other chemical mediators which are responsible for the allergic symptoms that occur. Most allergic reactions to sesame are caused by oleosins, the proteins in sesame.
Symptoms:
Individuals with a sesame allergy may experience a variety of symptoms that can range from mild to severe. The symptoms may include itchiness of the throat or mouth, generalized itching (i.e., pruritus), hives (i.e., urticaria), swelling (i.e., angioedema), nausea, vomiting, diarrhea, abdominal pain, flushing of the face, hoarseness, coughing, wheezing, and/or shortness of breath
A person with a severe reaction to sesame may experience anaphylaxis. Anaphylaxis is a life-threatening reaction that requires immediate medical attention. Some of the symptoms of anaphylaxis may include hives, shortness of breath, generalized itching, swelling, wheezing, fainting, dizziness, drop in blood pressure, rapid heartbeat, and/or cardiac arrest. Individuals who experience anaphylaxis due to sesame should carry a self-injectable epinephrine device (e.g., EpiPen, Auvi-Q, Adrenaclick) with them at all times. If the self-injectable epinephrine device is used, they should go immediately to the closest emergency room.
In packaged foods manufactured prior to January 1, 2023, sesame may appear undeclared in ingredients such as flavors or spice blends.
Some foods that may contain sesame:
Asian cuisine – Sesame oil is commonly used in cooking
Diagnosis: Skin Prick Testing – A safe and low-risk test in which the skin is lightly pricked with a suspected allergen. This can result in a raised bump or hive, with more severe reactions pointing to a greater likelihood of an allergy.
Blood Test – Measures the amounts of IgE antibodies (i.e., “allergy” antibodies) that the immune system has deployed as an allergic response to sesame.
Like tree nut allergies, sesame allergies are sometimes cross-reactive. In other words, if you are allergic to sesame, you could be allergic to similar seeds and nuts.
Treatment:
Mild allergic reactions to sesame can be treated with antihistamines. Systemic reactions with generalized symptoms needs to be treated with injectable epinephrine.
Prevention:
Diligent reading of the labels and strict avoidance of exposure to all sesame-containing products is necessary in order to prevent allergic reactions to sesame. Most patients with sesame allergy unfortunately do not “outgrow” the sensitivity.
If you suffer from or suspect a sesame allergy or any other type of allergy, the board certified allergists at Black & Kletz Allergy have the expertise in diagnosing and treating your condition. We treat both pediatric and adult patients and have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. We have on-site parking at each location and both the Washington, DC and McLean, VA offices are Metro accessible. Please either call us for an appointment or you may alternatively click Request an Appointment and we will respond within 24 hours by the next business day. The allergy specialists at Black & Kletz Allergy have been treating allergy, asthma, and immunology patients in the Washington, DC metropolitan area for more than 5 decades and we strive to provide state-of-the-art allergy care to its residents and visitors.
It is quite common for individuals to be allergic to mold, particularly in the Washington, DC, Northern Virginia, and Maryland metropolitan area. Not only is the humidity elevated in this region, but Washington, DC was built on a swamp. In the Spring, it rains quite often contributing to an increase in moisture and thus mold. In the Summer, the metro area tends to be hot and humid which is ideal for mold growth. During the Fall, the leaves fall from the trees and get wet which is the perfect environment for the development and progression of mold. Even during the Winter mold can flourish particularly since mold lives both indoors and outdoors. In the home, molds tend to be more prevalent in bathrooms, kitchens, and basements, where moisture is more common. It is interesting to note that some molds can survive in very arid environments such as a desert. Any way you slice it, mold is year-round problem for residents and visitors of the Washington, DC metropolitan area.
Mold is a fungus that grows in the form of multicellular filaments that are known as hyphae. There are over 400,000 types of molds. Mildew is also a fungus that closely resembles mold. Mold typically looks fuzzy in appearance while mildew characteristically is flat in appearance. The color of mold tends to be black, blue, green, or red whereas the color of mildew tends to be white, brown, or gray. Mold and mildew produce undesirable odors that many people find offensive or downright problematic as they can cause “sicknesses” to those exposed. Fungi that grow in a single-celled environment are called yeasts. Regardless of their characteristics, mold, mildew, and yeast can all play havoc to individuals who are either sensitive or allergic to them. Regarding allergies to mold, mildew, yeast, and fungi, an allergy to any one of them is generally grouped into one category as “allergy to mold,” as opposed to an allergy to mildew, an allergy to yeast, or an allergy to fungi.
Molds produce tiny microscopic which are their reproductive structures. The diameter of a mold spore generally varies between 3 to 45 microns which is less than half the width of a typical human hair. The mold spores begin are released into the air and since they are tiny in size, they are able to float in the air, where they can be easily inhaled by sensitive individuals. Mold spores flourish in any milieu with a constant source of moisture. As mold grows, the tiny spores begin to undergo chemical reactions that allow them to consume nutrients and further replicate. These chemical reactions produce fumes which are released into the atmosphere. These fumes are responsible for the unpleasant musty odor that everyone is familiar with.
Mold generally can cause annoying symptoms in 4 different ways. The first is from a true allergy to the mold. The most common type of symptoms from mold allergy are the kinds of symptoms one may experience from other environmental allergens such as dust mites, pollens, pets, or cockroaches. These allergic rhinitis (i.e., hay fever) and allergic conjunctivitis (i.e., eye allergies) symptoms may include sneezing, runny nose, post-nasal drip, nasal congestion, itchy throat, sore throat, sinus headaches, snoring, itchy eyes, watery eyes, puffy eyes, and/or redness of the eyes. Severely affected individuals as well as asthmatics may also develop asthma symptoms or an exacerbation of their asthma which may include wheezing, chest tightness, coughing, and/or shortness of breath. The diagnosis of mold allergy necessitates a comprehensive history and physical examination in conjunction with allergy testing (skin tests and/or blood tests). The treatment of mold allergy always begins with prevention. Avoiding mold is always preferable if at all possible. Some of the ways to help reduce mold exposure may include decreasing outdoor activities when mold counts are high, repairing any leaks, lowering the humidity, using a dehumidifier, using air conditioner with a HEPA filter, removing carpets in locations where they are in danger of becoming wet, and masking when engaging in yardwork. The treatment of mold allergy consists of allergy medications (e.g., antihistamines, decongestants, nasal corticosteroids, nasal antihistamines, leukotriene antagonists, eye drops, asthma inhalers) to help relieve one’s symptoms. Allergy shots (i.e., allergy injections, allergy immunotherapy, allergy desensitization, allergy hyposensitization) are extremely effective in the treatment of mold allergy. They are effective in 80-85% of the patients who receive them. Allergy injections have been given in the U.S. for more than 100 years as they get more to the root of the underlying problem by allowing a patient to develop protective antibodies against mold as well as other allergens such as dust mites, pollens, pets, and/or cockroach.
An unusual allergy to mold exists in roughly 1-2% of individuals with asthma. These individuals have an allergic reaction to a specific type of mold known as Aspergillus fumigatus. Similarly, between 2-15% of children with cystic fibrosis have the same reaction to this same mold. Asthmatic and cystic fibrosis patients that react to this mold have a condition known as allergic bronchopulmonary aspergillosis (ABPA). The symptoms of ABPA are similar to that of asthma except they may also cough up sputum with brownish flecks and they may also have a mild low-grade fever. Such patients should be worked up for ABPA via X-rays/CT scans, pulmonary function tests, sputum cultures, blood tests, and allergy skin tests. The treatment of ABPA usually involves the use of medications to treat asthma with the possible addition of oral corticosteroids and/or antifungal medications.
The second way mold can affect an individual is from a non-allergic irritant reaction. Molds can release substances known as volatile organic compounds (VOC’s) which can irritate skin and mucus membranes inside the mouth, nose, and eyes resulting in burning sensation of the skin, itchy throat, runny nose, itchy eyes, watery eyes, and/or cough. Avoidance is the best way to prevent irritant reactions. Using air filters may also be of help.
The third manner in which a mold can cause bothersome symptoms is via a toxic reaction usually by way of inhaled or ingested toxic compounds called mycotoxins, which are produced by the mold. The molds that produce mycotoxins can pose serious health risks to humans and animals. Some studies claim that the exposure to high levels of mycotoxins can result in neurological complications and prolonged exposure may be particularly harmful. The research on the health effects of these types of molds is somewhat controversial and it has not been conclusive. The term “toxic mold” refers to molds that produce mycotoxins, such as Stachybotrys chartarum and not to all molds in general. Mold remediation by a professional mold remediation service is the best way to remedy this situation.
The fourth method in which a mold can cause unwanted symptoms is by causing an infection. This results from the growth of a pathogenic mold within the body. The most common way that molds/fungi cause infections is through the skin. It should be noted that different types of molds/fungi can cause infections in other organ systems which may lead to gastrointestinal, respiratory, and/or neurological problems. Antifungal medications and occasionally other medications are used in order to eliminate the fungal infection.
The board certified allergy doctors at Black & Kletz Allergy will promptly respond to any questions regarding mold allergy or any other allergic or immunologic disorders. We have been treating mold allergies for more than 50 years and have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. We have been serving the Washington, DC, Northern Virginia, and Maryland metropolitan area for a long time and treat both pediatric and adult patients. All 3 offices at Black & Kletz Allergy offer on-site parking and the Washington, DC and McLean, VA offices are Metro accessible. There is a free shuttle that runs between our McLean, VA office and the Spring Hill metro station on the silver line. If you are concerned that you may have a mold allergy or any other allergy, asthma, sinus, skin, or immunology problem(s), please call us to schedule an appointment. You may also click Request an Appointment and we will answer within 24 hours by the next business day. At Black & Kletz Allergy, we strive to improve the quality of life in allergic and asthmatic individuals in a professional and compassionate environment.
Nasal polyps (i.e., nasal polyposis) are soft, benign growths that develop from the lining of the sinuses and nasal cavity. Approximately 4-5% of the general population has nasal polyps. They look like glistening moist grapes and are typically in the shape of teardrops. These new growths result from chronic inflammation of the tissues inside the nasal and sinus cavities. When the nasal polyps grow large enough, they may obstruct the nasal passages which will block the flow of air through the nose. The mechanical obstruction may also block the passage of secretions from the sinuses into the nose which may result in the predisposition of individuals to develop recurrent or chronic sinus infections.
CAUSES:
Any condition which ends in chronic inflammation inside the sinuses and nose may lead to the formation of nasal polyps. Some of these conditions may include:
1. Allergic sensitivity to indoor or outdoor environmental allergens [allergic rhinitis (i.e., hay fever)] mediated by an the IgE antibody and elevated levels of interleukin 5 (IL-5) cytokine.
2. Chronic sinus infections from bacteria such as Staphylococci as seen in chronic rhinosinusitis with nasal polyposis (CRSwNP).
3. Allergic response to fungal organisms in the inhaled air which is called allergic fungal rhinosinusitis (AFRS).
4. Systemic inflammatory disorders such as aspirin exacerbated respiratory disease (AERD) and cystic fibrosis (CF). Aspirin exacerbated respiratory disease is also called Samter’s triad because it consists of 3 features: asthma, nasal polys that re-occur, and an intolerance to aspirin and NSAID’s (nonsteroidal anti-inflammatory drugs). Between 6% and 48% of individuals with cystic fibrosis develop nasal polyps, so cystic fibrosis should be entertained in anyone who presents with nasal polyps.
5. Eosinophil (i.e., a type of white blood cell) disorders such as eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as Churg-Strauss syndrome.
6. Chronic irritation from smoke, strong odors, and pollutants in the air.
7. Immunodeficiencies such as common variable immunodeficiency, selective IgA deficiency, and primary ciliary dyskinesia
SYMPTOMS:
The symptoms of nasal polyps usually include nasal congestion and a runny nose in the early stages. As time goes on, nasal congestion resulting in a difficulty in breathing through the nostril(s) may occur. The nasal congestion usually worsens as the size of the polyp increases. Other symptoms of nasal polyps may include post-nasal drip, facial pain, headache, decreased or loss of taste (i.e., ageusia) and/or smell (i.e., anosmia), and snoring.
DIAGNOSIS:
The diagnosis of nasal polyps is generally made by examining the nasal cavity with a light source. The presence of nasal polyps will be revealed by shiny, mobile, smooth, gray, and semi-translucent masses. These Inflammatory polyps are usually present in both nostrils. It is important to note that some neoplastic polyps may only be present on one side (i.e., in one nostril). Rhinoscopy is often utilized to visualize the nasal cavity. Imaging of the sinuses with a CT scan may be needed in order to estimate the extent of the polyposis and to plan for surgical removal, if indicated. Allergy testing (e.g., skin testing, blood testing) is often performed to check for environmental allergies. A sweat chloride test may also be performed particularly in children in order to rule out cystic fibrosis.
COMPLICATIONS:
Some complications may arise from having nasal polyps. The problems may include nose bloods (i.e., epistaxis), recurrent or chronic sinusitis, asthma exacerbations, obstructive sleep apnea/snoring, and rarely double vision (i.e., diplopia).
TREATMENT:
1. Intranasal corticosteroid sprays [e.g., Flonase (fluticasone), Nasonex (mometasone), Nasacort (i.e., triamcinolone), Rhinocort (i.e., budesonide), Nasarel (i.e., flunisolide), Xhance (fluticasone)] on a daily basis.
2. Short courses of oral corticosteroids can shrink nasal polyps.
3. Saline irrigation: High-volume, low-pressure nasal saline irrigations are safe and non-expensive. Irrigation increases the clearance of antigens, biofilms, and inflammatory mediators.
4. Topical antihistamine nasal sprays [e.g. olopatadine (Patanase), azelastine (Astelin)]
5. Irrigation or nebulization with anti-inflammatory agents such as budesonide or mometasone in cases of CRSwNP.
6. Allergy testing and allergy immunotherapy (i.e., allergy shots, allergy desensitization, allergy hyposensitization) with relevant inhaled environmental allergens is effective in the treatment of allergic rhinitis, allergic conjunctivitis (i.e., eye allergies), and asthma in 80-85% of the patients that take them.
7. Deposition of corticosteroid medications higher into the nasal cavity by exhalation devices such as Xhance (i.e., fluticasone).
8. Biologic medications such as dupilumab (i.e., Dupixent) given by injections under the skin every 2 weeks, omalizumab (i.e., Xolair) given under the skin every 4 weeks, or mepolizumab (i.e., Nucala) given under the skin every 4 weeks.
9. Aspirin desensitization for AERD.
10. Functional endoscopic sinus surgery (FESS) and excision of the nasal polyps, restoring the patency of the nasal cavity.
11. Polyps have a tendency to recur after surgery and/or aggressive allergy treatments and intranasal corticosteroids can delay or prevent the recurrence.
12. Placing tiny, corticosteroid-coated implants (e.g., Sinuva) in the sinuses.
PREVENTION:
The aggressive management of predisposing conditions such as allergic rhinitis, controlling one’s environment [i.e., reducing one’s exposure to offending allergens such as dust mites, molds, pollens, cats, dogs, and cockroaches, allergy medications, and allergy immunotherapy (i.e., allergy shots, allergy injections, allergy immunotherapy, allergy hyposensitization) may all work together to inhibit polyp formation. In addition, avoiding exposure to strong odors, chemicals, and smoke is important in order to diminish nasal irritation and excessive tissue growth.
Individuals with established chronic sinusitis may require antibiotics, nasal or sinus irrigations, and/or sinus surgery. Patients with a history of aspirin sensitivity should do better after desensitization to aspirin in terms of improved asthma control, as well as a reduction in the recurrence of nasal polyps.
The board certified allergists at Black & Kletz Allergy have been diagnosing and treating both children and adults in the Washington, DC, nNorthern VA, and Maryland metropolitan area for over 50 years. We have offices in Washington, DC, McLean, VA (Tysons Corner, VA), and Manassas, VA. There is on-site parking at all of the offices. The Washington, DC and McLean, VA office locations are Metro accessible and there is a free shuttle that runs between our McLean office and the Spring Hill metro station on the silver line. The allergy doctors at Black & Kletz Allergy specialize in all types of allergic conditions including nasal polyps, hay fever, asthma, sinus disease, hives (i.e., urticaria), eczema (i.e., atopic dermatitis, swelling problems (i.e., angioedema), food and medication allergies, and immunological disorders. If you would like to schedule an appointment, please call us or alternatively you can click Request an Appointment and we will respond back to you within 24 hours on the next business day. We look forward to providing you with comprehensive state-of the-art allergy care in a friendly and professional environment.
 A landmark study published in 2015 called “Learning Early About Peanut Allergy (LEAP),” revolutionized our understanding of the development of peanut allergy in children and transformed the guidance that pediatricians and allergists/immunologists give to parents about when to introduce peanut foods to children at high risk for food allergies.
A landmark study published in 2015 called “Learning Early About Peanut Allergy (LEAP),” revolutionized our understanding of the development of peanut allergy in children and transformed the guidance that pediatricians and allergists/immunologists give to parents about when to introduce peanut foods to children at high risk for food allergies. Christmas tree syndrome is a relatively new term that is used to describe allergies to Christmas trees, whether they are real or artificial. The allergen can be the tree itself or it can be something that is on the surface of the tree.
Christmas tree syndrome is a relatively new term that is used to describe allergies to Christmas trees, whether they are real or artificial. The allergen can be the tree itself or it can be something that is on the surface of the tree.
 Corn (i.e., maize) is a popular staple food worldwide, providing essential nutrients such as vitamins, minerals, and fiber. Corn is also a common component of processed foods. Despite its nutritional value and popularity, for those individuals with corn allergies or corn intolerance, consuming corn or corn-derived products may lead to adverse health effects.
Corn (i.e., maize) is a popular staple food worldwide, providing essential nutrients such as vitamins, minerals, and fiber. Corn is also a common component of processed foods. Despite its nutritional value and popularity, for those individuals with corn allergies or corn intolerance, consuming corn or corn-derived products may lead to adverse health effects. Snoring is not an uncommon symptom in patients with
Snoring is not an uncommon symptom in patients with  The Eustachian tube is a small canal that connects the middle ear to the back of the nose and upper throat. It is normally closed but opens when we swallow, yawn, or chew.
The Eustachian tube is a small canal that connects the middle ear to the back of the nose and upper throat. It is normally closed but opens when we swallow, yawn, or chew. The term “chronic sinusitis” is defined as an inflammation of the sinus or sinuses lasting more than 12 weeks in duration. The inflammation can be of any etiology however it is implied and commonly agreed upon that infection is the primary cause of chronic sinusitis. In order to understand chronic sinusitis, it is important to know the anatomy of a sinus. A sinus is a cavity in any organ or tissue, but in reference to allergies, it is a cavity in the skull and often referred to a “paranasal sinuses.” There are 4 paired sinuses in the cranial bones. They are named for their location with regards to the head and face. The names of the sinuses include the frontal, ethmoid, sphenoid, and maxillary sinuses. The frontal sinuses are located in the forehead region above the eyes. The ethmoid sinuses are situated between the eyes on each side of the upper nose. The sphenoid sinuses are positioned behind the eyes and bridge of the nose and lie in the deeper areas of the cranium. The maxillary sinuses are located on either side of the nostrils in the cheekbone areas.
The term “chronic sinusitis” is defined as an inflammation of the sinus or sinuses lasting more than 12 weeks in duration. The inflammation can be of any etiology however it is implied and commonly agreed upon that infection is the primary cause of chronic sinusitis. In order to understand chronic sinusitis, it is important to know the anatomy of a sinus. A sinus is a cavity in any organ or tissue, but in reference to allergies, it is a cavity in the skull and often referred to a “paranasal sinuses.” There are 4 paired sinuses in the cranial bones. They are named for their location with regards to the head and face. The names of the sinuses include the frontal, ethmoid, sphenoid, and maxillary sinuses. The frontal sinuses are located in the forehead region above the eyes. The ethmoid sinuses are situated between the eyes on each side of the upper nose. The sphenoid sinuses are positioned behind the eyes and bridge of the nose and lie in the deeper areas of the cranium. The maxillary sinuses are located on either side of the nostrils in the cheekbone areas. Allergic reactions to sesame are increasing in incidence over the past several years. Sesame is the 9th most common food allergy among children and adults. Approximately 0.23% of the U.S population are allergic to sesame. Although 0.23% seems like a small number, the National Institute of Health’s (NIH) researchers estimate that 17% of food-allergic children have a sesame allergy.
Allergic reactions to sesame are increasing in incidence over the past several years. Sesame is the 9th most common food allergy among children and adults. Approximately 0.23% of the U.S population are allergic to sesame. Although 0.23% seems like a small number, the National Institute of Health’s (NIH) researchers estimate that 17% of food-allergic children have a sesame allergy.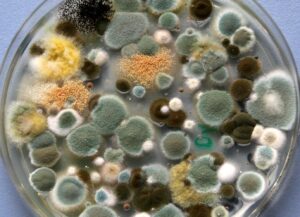 It is quite common for individuals to be allergic to mold, particularly in the
It is quite common for individuals to be allergic to mold, particularly in the  Nasal polyps (i.e., nasal polyposis) are soft, benign growths that develop from the lining of the sinuses and nasal cavity. Approximately 4-5% of the general population has nasal polyps. They look like glistening moist grapes and are typically in the shape of teardrops. These new growths result from chronic inflammation of the tissues inside the nasal and sinus cavities. When the nasal polyps grow large enough, they may obstruct the nasal passages which will block the flow of air through the nose. The mechanical obstruction may also block the passage of secretions from the sinuses into the nose which may result in the predisposition of individuals to develop recurrent or chronic sinus infections.
Nasal polyps (i.e., nasal polyposis) are soft, benign growths that develop from the lining of the sinuses and nasal cavity. Approximately 4-5% of the general population has nasal polyps. They look like glistening moist grapes and are typically in the shape of teardrops. These new growths result from chronic inflammation of the tissues inside the nasal and sinus cavities. When the nasal polyps grow large enough, they may obstruct the nasal passages which will block the flow of air through the nose. The mechanical obstruction may also block the passage of secretions from the sinuses into the nose which may result in the predisposition of individuals to develop recurrent or chronic sinus infections.








